
Welcome from EUS-AAEM
The Emergency Ultrasound Section of the American Academy of Emergency Medicine (EUS-AAEM) was founded to foster the professional development of its members and to educate them regarding point-of-care ultrasound. This group will serve as a venue for collaboration among medical students, residents and practitioners who are interested in point-of-care ultrasound. The purpose of our group is to augment the knowledge and expertise of all emergency medicine specialists and to advocate for patient safety and quality care by endorsing bedside ultrasound. Membership is not limited to fellowship trained physicians. All emergency medicine practitioners passionate about ultrasound are welcome to join and participate.
We are proud to publish our e-newsletter with original contributions from many of our members. We encourage all members to submit for future editions. Topics include but are not limited to educational, community focus, interesting cases, resident and student section, and adventures abroad.
For more information, visit our webpage.
In this Issue
- President’s Message
- Opportunities to Get Involved
- Medical Student Section
- Resident Section
- Ultrasound Saves
- Fellows Section
- Procedures Section
President’s Message
Hello fellow EUS-AAEM members,
What a year 2023 has been! Several projects are underway with the AAEM Emergency Ultrasound Section this year, and I am thrilled to give you the following updates.
During the successful SA23 in New Orleans this spring, our Section introduced both our SonoSleuthing medical student competition and Ultrasound Photo Poster competitions! We had a huge turnout to our Meet & Greet with our new Council members, and the various lectures and small group sessions led by our members were all captivating. We are preparing several offerings for SA24 in Austin, TX, in April 2024, and hope to see you there!
Our newly re-imagined third season of the Unmute Your Probe virtual lecture series has kicked off! This year we are teaching various Ultrasound Administration topics such as Coding & Billing, as well as covering the required content needed to pass the Focused Practice Designation for Advanced Emergency Medicine Ultrasonography (FPD-AEMUS) exam in the upcoming March 2024 testing cycle. But for those not taking the exam, do not forget that the past two full years worth of Basic and Advanced ultrasound lectures are all still available online for free to EUS-AAEM members, so check out those webinar archives on our webpage and even earn some CME!
The POCUS Report has continued to publish engaging and thought-provoking articles. We are growing our Speaker’s Bureau with several medical student EM interest group lectures currently being planned. And we are actively advertising for our Regional Hands-On Course initiative, a unique program where community EM sites that lack local ultrasound resources can train their staff in a carefully designed ultrasound course which we tailor to your specific needs and bring to your shops.
New this year, we have created a Research Grant that will accept its first round of applicants this fall! Keep an eye on our webpage for the application link and more information to be posted.
We welcome everyone who wants to get involved with the Section (https://www.aaem.org/get-involved/sections/eus/)! Please contact our staff liaison Kathy Uy at kuy@aaem.org, and she will direct you toward whichever project you are interested in.
Back in 2018, I wandered into an EUS-AAEM meeting at SA as a hesitant intern who was newly nerdy about Ultrasound. Little did I know the power of AAEM’s members in getting young passionate learners involved in the process and teaching us principles and leadership skills beyond what our medical training alone can offer. Here I have found a close-knit group of like-minded individuals, who have mentored and guided me through my fellowship into attending life. I am honored and forever grateful to serve as your Chair this year, and I cannot wait to see where we can take this Section next!
Neha Bhatnagar, MD, FAAEM FPD-AEMUS
Chair, EUS-AAEM
nbhatnagar.md@gmail.com
@nbhatngar_md
Opportunities to Get Involved
Help Wanted: Speakers
The Emergency Ultrasound Section is looking for interested residents, fellows and faculty to speak with medical school Emergency Medicine Interest Groups and Ultrasound Interest Groups about the use of point of care ultrasound in the Emergency Department.
The section will provide a list of suggested topics to the Interest Groups, as well as providing you with several slide sets to use if you choose as a basis for lectures. This is a great opportunity for anyone interested in sparking interest in the next generation of Emergency Physicians in the use of point of care ultrasound in the Emergency Department! Interested physicians may sign up here.
An Opportunity for EMIGs
The American Academy of Emergency Medicine Emergency Ultrasound Section has an exciting new opportunity focused on providing emergency ultrasound education to groups like yours. The section has compiled a group of point of care ultrasound enthusiasts who are making themselves available to give virtual talks on a variety of emergency ultrasound topics. This is a great chance to get directed education on an exciting and ever expanding diagnostic topic directed to your group’s specific interest. If you think your group would be interested in taking advantage of this opportunity, please sign up through the sign-up link below.
Please designate your interest on this worksheet.
Medical Student Section:
Use of Ultrasound in the Diagnosis of Retinal Detachment
Benjamin Kowalske, MS-3, Clarice Callahan MS-4, Megan Coble, MS-3, Matthew Flannigan, DO, Dr. Daniel Ritter, MD, Jordan Johnson, MD
Michigan State University College of Human Medicine; Department of Emergency Medicine
Corewell Health Hospitals, Grand Rapids, MI
Introduction
Retinal detachment occurs when vitreous fluid enters and separates the neurosensory layer of the retina from the outer layer of epithelium.1 It classically presents as flashes of light and floaters in the visual fields. This may be accompanied by visual field deficits, often described as a “curtain” coming across the visual field, or decreased visual acuity. The lifetime prevalence of retinal detachment is 0.1%, and it can lead to blindness if not treated promptly.1,2 Risk factors include high myopia, ocular trauma, prior ocular surgery or posterior vitreous detachment, family history of retinal detachment, and increased age.1,3 The gold standard for diagnosing retinal detachment is a dilated funduscopic exam, but this is not always feasible in the emergency department (ED). Point-of-care ultrasound (POCUS) provides an effective alternative method to diagnose retinal detachment.2,4 A 2019 systematic review and meta-analysis found that ED providers achieved a 97% sensitivity and 92% specificity for detecting retinal detachment with POCUS.5
Case Presentation
A 64-year-old male with history of hypertension presented to the ED with worsening painless blurry vision in the left eye. The patient’s initial blood pressure was 208/140 mmHg and heart rate 105 beats per minute; vital signs were otherwise within normal limits. He described seeing blurred lines with his left eye beginning the previous day. This progressed to diffusely blurry vision in his left eye just prior to presentation in the ED. Visual acuity in his left eye was limited to light perception. His pupils were equal, round, and reactive to light, and his conjunctivae appeared grossly normal. The affected retina was unable to be visualized on a fundoscopic exam. POCUS was unavailable, so the patient underwent a computed tomography (CT) scan of his brain and an ophthalmology consultation. The CT showed no evidence of acute ischemic or hemorrhagic stroke. The ophthalmologist reviewed the CT and was concerned for retinal hemorrhage versus retinal detachment but was not available for face-to-face evaluation of the patient. He was therefore transferred to another emergency department where further evaluation for retinal detachment could occur. POCUS was completed by an ultrasound fellowship-trained emergency medicine physician which revealed a complete retinal detachment. An ophthalmologist reviewed the ultrasound images and agreed with the ED physician’s interpretation. The patient was scheduled for outpatient surgery to occur two days later.
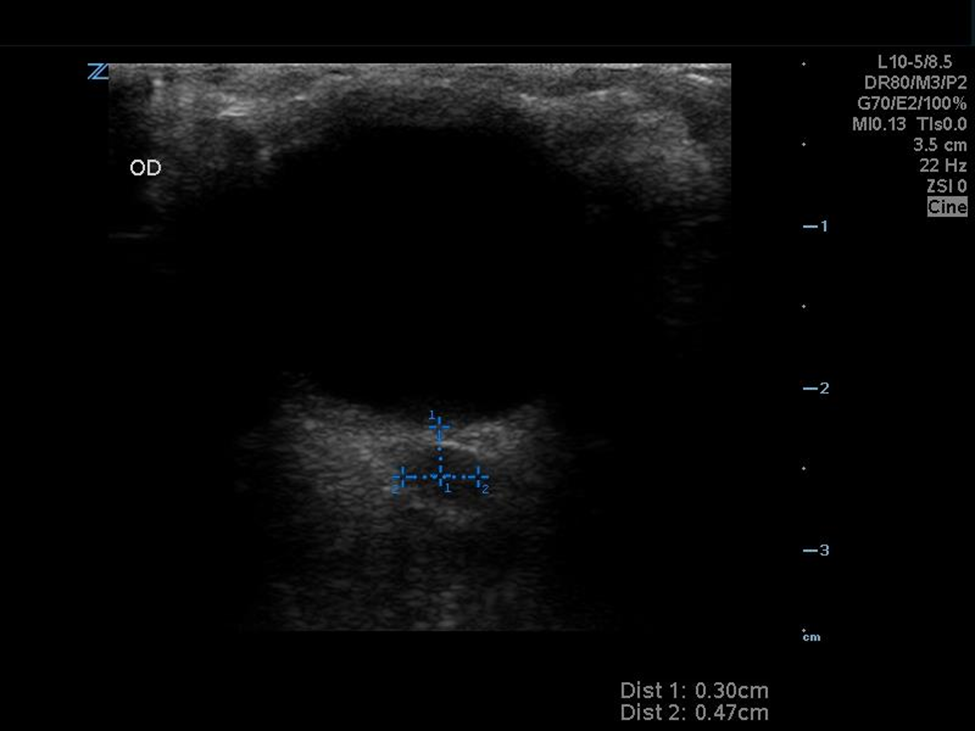
Image 1: Normal retinal ultrasound
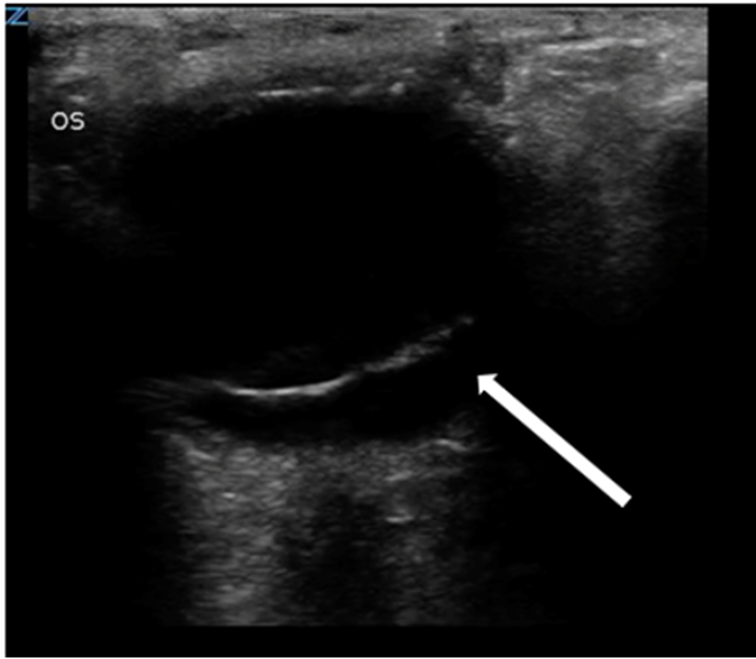
Image 2: POCUS was performed by an emergency physician, indicating a left retinal detachment with macular separation.
Discussion
POCUS is sensitive and specific for diagnosing retinal detachment.5 It is useful tool for the evaluation of patients with acute visual changes, providing a detailed view of ocular structures without requiring pupillary dilation, extensive subspecialty training, or ionizing radiation exposure.6 When compared to CT, POCUS is faster and more cost-effective for the diagnosis of retinal detachment. This case report highlights the importance of utilizing POCUS to make timely diagnosis of vision threatening conditions, such as retinal detachment, and reduce diagnostic uncertainty and unnecessary transfers.
Retinal detachment is an emergent condition that can result in permanent vision loss if left untreated. POCUS allows for rapid and accurate diagnosis of retinal detachment, with high sensitivity and specificity, making it an appealing tool for ED providers.5 A linear high-frequency transducer should be used when imaging the eye. Using an ocular preset is recommended to reduce exposing the eye to potentially harmful thermal energy. Retinal detachment appears on ultrasound as a thick, hyperechoic membrane that is lifted off the posterior surface of the globe.5 This membrane will appear tethered to the optic nerve, forming a “V” shape. Small retinal detachments can be more difficult to identify due to closer tethering to the back wall of the globe. It is therefore recommended to scan the eye in multiple axes. Having the patient move his or her eye side-to-side (after movement) can also help to highlight pathology within the eye.
Differentiating retinal detachment from posterior vitreous detachment (PVD) with POCUS can be challenging but is important due to differences in management. Unlike the urgency that is present with a retinal detachment, a “wait and see” approach is typically utilized with PVD. The largest point of differentiation between the two pathologies lies in the tethering of the membrane to the optic nerve. In PVD, the membrane is not tethered to the optic nerve and will move much more freely with eye movements. It is important to recognize that both pathologies can be present simultaneously, as a PVD can lead to a retinal detachment7.
Conclusion
This case highlights the utility of ocular ultrasound as a core POCUS modality that should be learned by acute care providers who may encounter patients with sudden vision loss. POCUS is highly sensitive and specific for diagnosing retinal detachment. It allows ED providers to rapidly make the diagnosis at bedside while reducing costs and exposure to ionizing radiation.5,6 As seen in our case, CT is not a preferred imaging modality for the detection of retinal pathology, and an expert-performed, dilated fundoscopic examination may not be feasible in all practice locations. Use of POCUS by the initial ED provider may have prevented the need for transfer in this case. Providing appropriate point-of-care ocular ultrasound training to ED providers offers the opportunity to improve efficiency, cost-effectiveness, and diagnostic accuracy for common retinal pathology.
References
- Kwok JM, Yu CW, Christakis PG. Retinal detachment. Can Med Assoc J. 2020;192(12):E312-E312. doi:10.1503/cmaj.191337
- Botwin A, Engel A, Wasyliw C. The use of ocular ultrasound to diagnose retinal detachment: a case demonstrating the sonographic findings. Emerg Radiol. 2018;25(4):445-447. doi:10.1007/s10140-018-1585-z
- Baker N, Amini R, Situ-LaCasse EH, et al. Can emergency physicians accurately distinguish retinal detachment from posterior vitreous detachment with point-of-care ocular ultrasound? Am J Emerg Med. 2018;36(5):774-776. doi:10.1016/j.ajem.2017.10.010
- Shinar Z, Chan L, Orlinsky M. Use of Ocular Ultrasound for the Evaluation of Retinal Detachment. J Emerg Med. 2011;40(1):53-57. doi:10.1016/j.jemermed.2009.06.001
- Gottlieb M, Holladay D, Peksa GD. Point‐of‐Care Ocular Ultrasound for the Diagnosis of Retinal Detachment: A Systematic Review and Meta‐Analysis. Carpenter CR, ed. Acad Emerg Med. 2019;26(8):931-939. doi:10.1111/acem.13682
- Lahham S, Shniter I, Thompson M, et al. Point-of-Care Ultrasonography in the Diagnosis of Retinal Detachment, Vitreous Hemorrhage, and Vitreous Detachment in the Emergency Department. JAMA Netw Open. 2019;2(4):e192162. doi:10.1001/jamanetworkopen.2019.2162
- Moon SY, Park SP, Kim YK. Evaluation of posterior vitreous detachment using ultrasonography and optical coherence tomography. Acta Ophthalmol. 2020;98(1):e29-e35. doi:10.1111/aos.14189
Resident Section:
Pulmonary Artery Compression Secondary to Ruptured Thoracic Aortic Dissection: A Rare Mimic of Pulmonary Embolism
Ochan Kwon, MD; Alexandra Bourlas, DO; Ashley Voroba, MD; Angelo Mascia, DO
Case Presentation
A 51-year-old male was brought to the Emergency Department after being found collapsed in his apartment. Per EMS, the patient was bradypneic, hypoxic, and with pinpoint pupils. EMS administered naloxone in the field, after which the patient became more alert with improved respirations. Upon arrival to the ED, the patient’s initial vital signs were stable and he complained of chest pain with shortness of breath. On initial exam, the patient had clear lungs on auscultation without signs of respiratory distress, but eventually became diffusely diaphoretic and tachypneic. He was found to be hyperkalemic to 7.4 mEq/L with an elevated lactic acid of 3.8 mmol/L on venous blood gas. Shortly after, the patient became bradycardic and then went into PEA arrest. ROSC was obtained after three rounds of CPR, during which bedside echocardiography demonstrated a “D-sign” (figure 1), significant right ventricular and atrial dilation (figures 2 & 3), paradoxical septal wall motion (figure 2), and a plethoric IVC (figure 4).
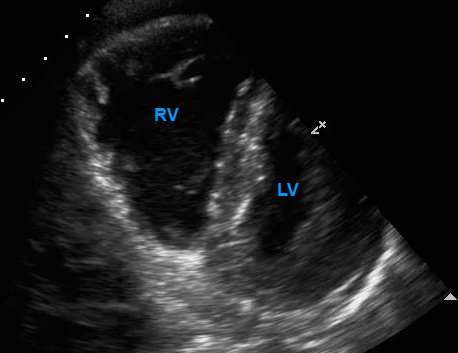
Figure 1: “D-sign”. In this parasternal short axis view of the heart, flattening of the interventricular septum resulting in the formation of a D-shape by the left ventricle can be seen. RV: Right ventricle; LV: Left ventricle.
Figure 2: Right ventricular dilation and paradoxical septal motion. In this parasternal short axis view of the heart, paradoxical motion of the interventricular septum towards the left ventricle during systolic contraction is shown.
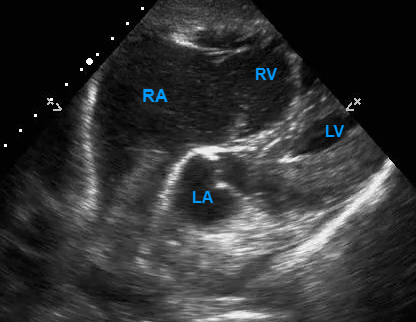
Figure 3: Dilation of the right ventricle and right atrium in this subxiphoid view of the heart. Note that the left atrium appears to be pushed towards the right atrium, possibly due to external compression by the ascending aorta. RV: Right ventricle; RA: Right atrium, LV: Left ventricle; LA: Left atrium.
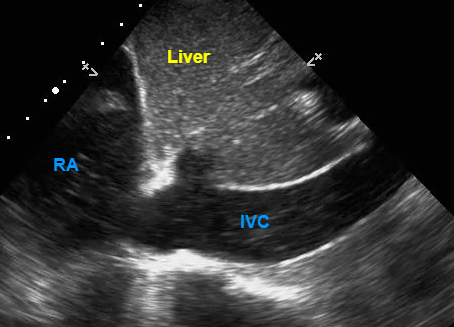
Figure 4: Plethoric IVC. Dilated IVC with minimal respiratory variation is shown. IVC: Inferior vena cava; RA: Right atrium.
Given this episode of sudden PEA in the setting of significant right heart strain visualized on ultrasound, the decision was made to administer alteplase (50mg IV push followed by 50mg IV infusion at a rate of 25 mg/hour) for suspected pulmonary embolism. Norepinephrine infusion was started to maintain blood pressure and the patient was sent for CT angiography of the chest. In the CT suite the patient again developed PEA arrest, and ROSC was achieved with CPR. The CTA chest showed a dissection of the ascending aorta with a contained rupture, which caused marked extrinsic compression primarily on the main and left proximal pulmonary arteries, as well as the left atrium and pulmonary veins (figure 5). A dilated right ventricle and atrium with marked underfilling of the left ventricle was shown as well. Once imaging results were received, the patient was administered tranexamic acid as a reversal agent for alteplase. While awaiting transportation to an outside facility for cardiothoracic surgery evaluation, the patient again became bradycardic and hypotensive despite administration of atropine and multiple vasopressors. The patient developed asystole and despite multiple attempts at resuscitation, the patient died.
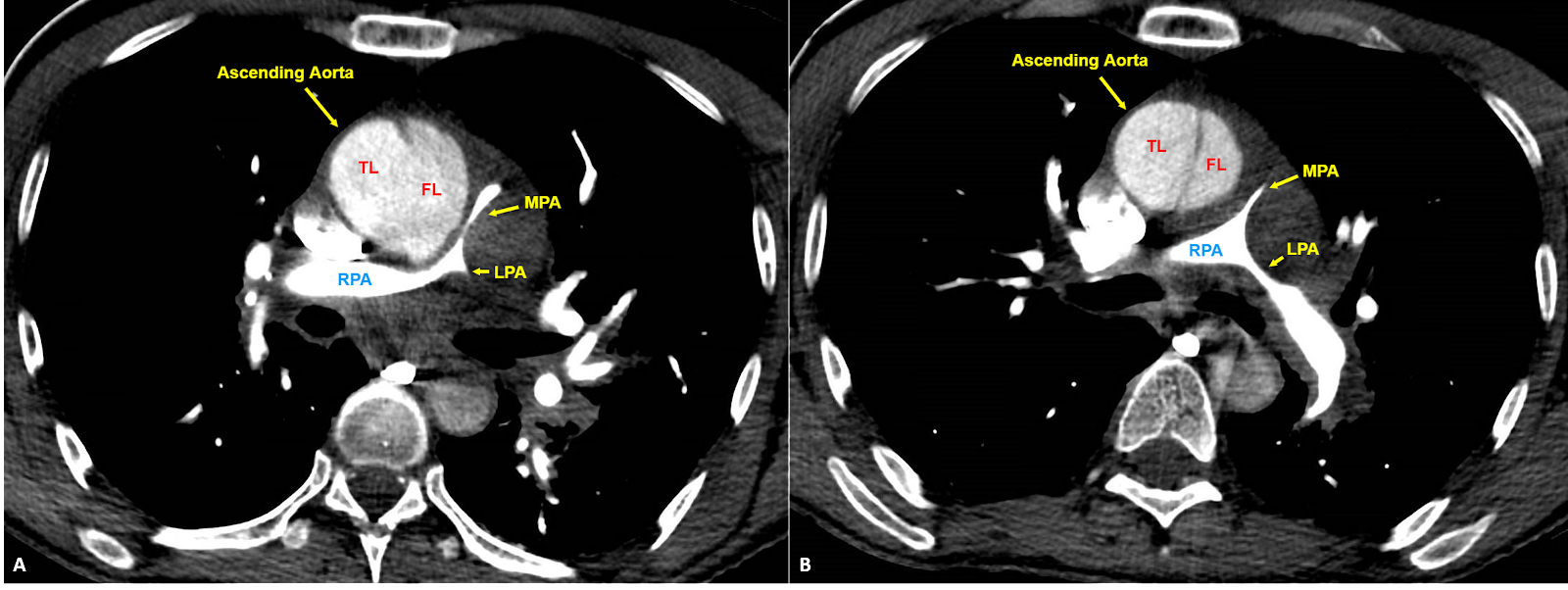
Figure 5: A. Dissection of the ascending aorta with visible extravasation of contrast between true and false lumens due to rupture or penetrating ulcer. Contained rupture can be seen compressing the main and left pulmonary arteries resulting in visible stenosis. B. More superior slice showing a clear intimal flap within the ascending aorta and compression of the main pulmonary artery. TL: True lumen; FL: False lumen; MPA: Main pulmonary artery; LPA: Left pulmonary artery; RPA: Right pulmonary artery.
Discussion
The right heart, specifically the right ventricle (RV), has anatomic differences compared to the left ventricle (LV) that make it particularly vulnerable to acute changes in afterload (3). Compared to the LV’s thick walls, the walls of the RV are thinner and much more compliant, allowing for overfilling with higher pressures. As a result, any acute increase in RV afterload and outflow resistance leads to right ventricular pressure overload, dilation of the compliant RV, and contractile dysfunction (13). This can be visualized on ultrasound with the “D-sign”, which refers to the D-shaped structure of the LV formed from the bowing of the interventricular septum away from the overloaded RV in the parasternal short axis view. In this case, POCUS during PEA arrest found signs of right heart strain such as “D-sign”, paradoxical septal motion, and dilation of the right ventricle and atrium in the setting of acute hemodynamic instability, leading to a presumed diagnosis of massive PE. However, there was no evidence of PE seen on CT imaging. Instead, the right ventricular strain appeared to be secondary to extrinsic compression of the pulmonary artery by a dissection of the ascending aorta with a contained rupture. Regardless, it is likely that the resulting combination of impaired cardiac contractility, cardiogenic shock, and dissection of the ascending aorta with possible concomitant myocardial infarction led to this patient’s PEA arrest.
How can we utilize POCUS to help us in the diagnosis of PE? Prior large-scale meta-analyses have shown that transthoracic echocardiography is highly specific, but poorly sensitive, in the diagnosis of PE for patients with high clinical suspicion (7); furthermore, focused cardiac ultrasound has proven useful for ruling out PE in patients with abnormal vital signs (4). In addition, abnormal septal motion, when found via physician-performed ultrasonography, has been shown to be highly specific for diagnosing PE (2, 7). Findings of right heart strain on POCUS led our team to suspect PE as a likely cause for this patient’s cardiac arrest. In fact, 36% to 53% of PE-related cardiac arrests present with PEA (12). However, this patient was found to have a different cause of increased right heart strain, a dissection of the ascending aorta with a contained rupture causing direct extrinsic compression of the pulmonary artery and left atrium. Therefore, it is crucial to consider a broad differential when evidence of right heart strain is found using POCUS.
This patient’s numerous complications involving the ascending aorta fall under acute aortic syndrome (AAS), an umbrella term that encompasses several conditions including complete or incomplete aortic dissection, intramural hematoma, and penetrating aortic ulcer (15). One particularly rare complication of AAS is pulmonary artery obstruction secondary to extrinsic mass effect caused by aortic compression. In fact, chronic thoracic aortic aneurysms have been previously shown to compress and obstruct the pulmonary artery leading to pulmonary hypertension, cor pulmonale, and right heart failure (1, 14). On the other hand, there have been multiple reports of acutely ruptured thoracic aortic dissections leading to extravasation of blood into the surrounding interstitial space, with the resulting hematoma shown to compress the pulmonary artery (8, 9, 10, 11). Other cases describe the contained rupture of a thoracic aortic dissection (5), as well as the contained rupture of a thoracic aortic aneurysm (6), both of which caused compression of the adjacent pulmonary artery. Regardless of the cause, an acute obstruction of the proximal pulmonary artery via extrinsic compression can lead to an abrupt increase in right ventricular afterload and symptoms of acute RV dysfunction that mimic a large central PE. In the case of our patient, we hypothesize that a dissection of the ascending aorta was complicated by a rupture or penetrating ulceration of the intimal flap leading to an acutely thrombosed false lumen; this segment of contained rupture expanded and caused significant extrinsic compression of the main and proximal left pulmonary arterial segments as well as the left atrium (figure 5). Extrinsic compression of the pulmonary artery and left atrium causing acutely symptomatic right ventricular failure is an exceedingly rare complication of aortic dissection.
Ultrasound findings of right heart strain have commonly been misconstrued to be pathognomonic for pulmonary pathology, classically PE. However, it is important to consider a broad differential for right heart strain particularly in an unstable patient presenting with chest pain. Here we demonstrate a case where findings of right heart strain on POCUS during cardiac arrest were not due to massive PE. While rare, complications of acute aortic syndrome can lead to extrinsic compression of pulmonary arteries and acute right ventricular failure, mimicking the presentation of PE.
References
- Abe T, Kamikubo Y, Taneichi T, Terada T, Sugiura J, Sakurai T, Tsuboi N, Sakurai H. Right heart failure secondary to compression of the right pulmonary artery by a large proximal aortic aneurysm. Circulation. 2013 Oct 1;128(14):1588-9.
- Alerhand S, Sundaram T, Gottlieb M. What are the echocardiographic findings of acute right ventricular strain that suggest pulmonary embolism? Anaesth Crit Care Pain Med. 2021 Apr;40(2):100852.
- Bryce YC, Perez-Johnston R, Bryce EB, Homayoon B, Santos-Martin EG. Pathophysiology of right ventricular failure in acute pulmonary embolism and chronic thromboembolic pulmonary hypertension: a pictorial essay for the interventional radiologist. Insights Imaging. 2019 Feb 13;10(1):18.
- Daley JI, Dwyer KH, Grunwald Z, Shaw DL, Stone MB, Schick A, Vrablik M, Kennedy Hall M, Hall J, Liteplo AS, Haney RM, Hun N, Liu R, Moore CL. Increased Sensitivity of Focused Cardiac Ultrasound for Pulmonary Embolism in Emergency Department Patients With Abnormal Vital Signs. Acad Emerg Med. 2019 Nov;26(11):1211-1220.
- Decroix A, Van Damme H, Creemers E, Defraigne JO. New Type A Aortic Dissection after a Chronic Type B Dissection, Compressing the Pulmonary Artery: A Case Report. Ann Vasc Surg. 2019 Oct;60:474.e11-474.e13.
- Felix AS, Alves LA, Felipe AR, Costa ALC, Segalote RC, Zappa MB, Camargo GC. Pulmonary Artery Compression and Invasion by a Ruptured Giant Thoracic Aortic Aneurysm: A Rare Presentation. CASE (Phila). 2018 May 4;2(5):201-206.
- Fields JM, Davis J, Girson L, Au A, Potts J, Morgan CJ, Vetter I, Riesenberg LA. Transthoracic Echocardiography for Diagnosing Pulmonary Embolism: A Systematic Review and Meta-Analysis. J Am Soc Echocardiogr. 2017 Jul;30(7):714-723.e4.
- Kim DH, Ryu SW, Choi YS, Ahn BH. Aortic dissection presenting with secondary pulmonary hypertension caused by compression of the pulmonary artery by dissecting hematoma: a case report. Korean J Radiol. 2004 Apr-Jun;5(2):139-42.
- Liu Y, Guo S, Zhu H, Wang Z, Yu X. Aortic dissection associated with right pulmonary artery compression. Postgrad Med J. 2012 Sep;88(1043):554-5.
- Masuo M, Takano H, Takamoto S, Tanaka J, Kitamura S, Saito T. Pulmonary artery obstruction caused by thoracic aortic dissection: a case with unique pathological findings. Circ J. 2004 Apr;68(4):392-5.
- Miura S, Iba Y, Yamada A. Type A aortic dissection with pulmonary hypertension caused by pulmonary artery compression and acute mitral regurgitation. Eur J Cardiothorac Surg. 2018 Aug 1;54(2):404.
- Panchal AR, Bartos JA, Cabañas JG, Donnino MW, Drennan IR, Hirsch KG, Kudenchuk PJ, Kurz MC, Lavonas EJ, Morley PT, O’Neil BJ, Peberdy MA, Rittenberger JC, Rodriguez AJ, Sawyer KN, Berg KM; Adult Basic and Advanced Life Support Writing Group. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020 Oct 20.
- Pinsky MR. The right ventricle: interaction with the pulmonary circulation. Crit Care. 2016 Sep 10;20(1):266.
- Sugiyama H, Tohma R, Misato T, Okamoto K, Hayashi T, Tobe S, Matsuo T, Tsunemi K, Oka T, Tanimura N. Right heart failure caused by direct pressure of distal arch aneurysm. Gen Thorac Cardiovasc Surg. 2019 Feb;67(2):263-265.
- Vilacosta I, San Román JA, di Bartolomeo R, Eagle K, Estrera AL, Ferrera C, Kaji S, Nienaber CA, Riambau V, Schäfers HJ, Serrano FJ, Song JK, Maroto L. Acute Aortic Syndrome Revisited: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021 Nov 23;78(21):2106-2125.
The Use of POCUS in Diagnosing a Young Man With Bilateral Vision Loss
Emily Zhao, MD, Katia Johnston, MD and Victoria Gonzalez, MD
Cook County Health, Chicago, IL
Case
A 30-year-old male with no past medical history presented with bilateral blurry vision and eye pain. He was seen three weeks earlier in the emergency department and diagnosed with conjunctivitis. At that time he was discharged with eye drops. A week and half later, he started having bilateral eye pain with a headache and returned to the emergency department. He could visualize shapes in the right eye and finger count in the left eye. Intraocular pressures were 18 on the right and 17 on the left. On bedside ultrasound, there was a suspicion of bilateral retinal detachment. Ophthalmology was consulted in the emergency department and diagnosed the patient with Vogt-Koyanagi-Harada. He was started on steroids on discharge and followed up in the ophthalmology clinic where he was started on mycophenolate and mydriatics and his vision improved overtime.
Discussion
Vogt-Koyanagi-Harada or VKH is a bilateral granulomatous panuveitis with or without extraocular manifestations.[4] This is a rare disease that is usually found in young adults. The incidence of this disease varies by geography. In the United States, the incidence of VKH is approximately 1.5 to 6 per 1 million patients.[1] It also presents more commonly in Hispanic and Southeast Asian populations. The patients often present with blurry vision and headache. They could also have extraocular manifestations such as vitiligo, cranial nerve findings and other central nervous system findings.[2] On ultrasound, the findings are serous retinal detachments, vitreous opacities, subretinal septations, mild thickening of the sclera and/or episclera adjacent to areas of choroidal thickening.[3] In this patient’s ultrasound, he was found to have multiple serous retinal detachments bilaterally.
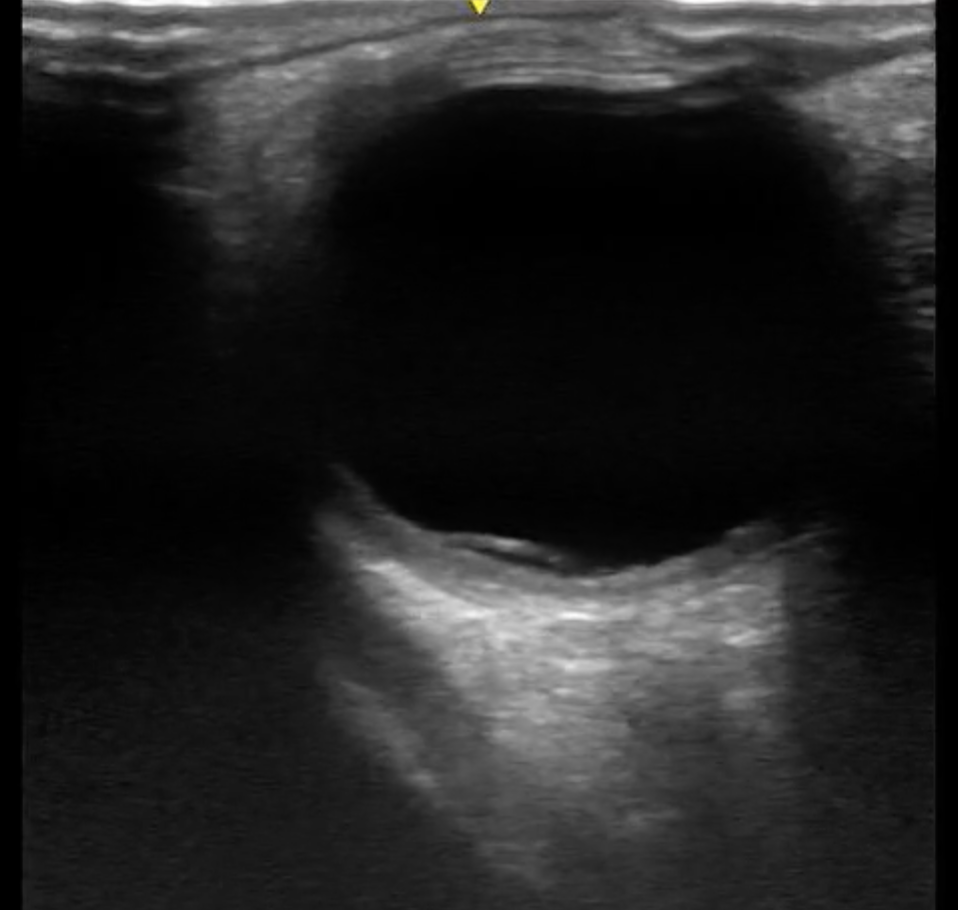
Figure 1: Right Eye

Figure 2: Left Eye
Conclusion
Point of care ocular ultrasound is a useful imaging tool to aid in the diagnosis of many eye diseases such as retinal detachment, lens dislocation, vitreous hemorrhage, central retinal artery occlusion. It can also help diagnose rare diseases such as VKH especially in patients with bilateral vision loss. Early detection in the emergency department and aggressive therapy are keys to maintaining good visual acuity.
References
- Lavezzo, Marcelo Mendes, et al. “Vogt-Koyanagi-Harada disease: review of a rare autoimmune disease targeting antigens of melanocytes.” Orphanet Journal of Rare Diseases 11 (2016): 1-21.
- Papaliodis G. Uveitis: Etiology, clinical manifestations, and diagnosis. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on August 10, 2023.)
- R R, Glick Y, Sharma R, et al. Vogt-Koyanagi-Harada disease. Reference article, Radiopaedia.org (Accessed on 10 Aug 2023) https://doi.org/10.53347/rID-27129
- Salcedo H. Vogt-Koyanagi-Harada Disease. American Academy of Ophthalmology, EyeWiki. June 2023. https://eyewiki.aao.org/Vogt-Koyanagi-Harada_Disease. Accessed August 10, 2023.
Ultrasound Saves:
A Stroke Saved – Left Ventricular Thrombus Identified with POCUS
Steve Lin MD, Victoria Gonzalez MD, and David Murray MD
Cook County Hospital, Chicago, IL
Case Vignette
A 55 year old male with HTN, CAD, and HFrEF due to ischemic cardiomyopathy (last recorded EF of 40%) presented with chest pain which woke him up from sleep and was associated with mild nausea. The pain was without radiation and was non-exertional and non-pleuritic in nature. There was no associated diaphoresis, difficulty breathing, dizziness, vomiting or presyncope. Patient also reported that his symptoms improved with exertion (for example, jumping up and down). The patient’s vital signs were within normal limits. His exam was significant for mild tenderness to palpation to the chest wall, but an unremarkable cardiopulmonary exam. His EKG was unchanged from prior and labs were unremarkable including two serial negative troponins.
Bedside echocardiography was performed with images shown below in Figures 1 and 2 demonstrating an echogenic mass in the apex of the left ventricle concerning for a thrombus. A comprehensive echocardiogram was ordered, and confirmed a 1.5 cm x 1.5 cm apical thrombus and was negative for a patent foramen ovale. Cardiology was consulted and the patient was started on a heparin drip, admitted, and ultimately transitioned to warfarin prior to discharge.

Figure 1 – Parasternal Long Axis View: LV Thrombus depicted by red arrow

Figure 2 – Apical 4 View: LV Thrombus depicted by red arrow
Discussion
Left Ventricular thrombus is a potential sequela of previous cardiac infarct (particularly an anterior infarct that involves the left ventricle)1 leading to stasis in the circulatory system. Circulatory stasis, in conjunction with inflammatory induced hypercoagulable states and damage to the myocardium/endocardium, increases the risk of LV thrombus. The incidence of LV thrombus seen in anterior infarction have steadily decreased over the years from as high as 46%, to recent reports as low as 17%, likely due to improvements in definitive treatment such as PCI.1,2 Other conditions that associated with LV thrombus include HFrEF (particularly with EF <40%), atrial fibrillation, and pulmonary veno-occlusive disease.1,3,4
The appearance of an LV thrombus seen on ultrasound can vary based on chronicity. Most commonly on ultrasound an LV thrombus appears homogeneous with a well-delineated border, and mobile (if acute). Myocardial thrombi are often seen at the apex of the left ventricle, as this is the most dependent region of the heart.3
The differential for an echogenic mass found in the left ventricle includes myxomas, cardiac tumors, vegetations (including bacterial and nonbacterial endocarditis), and anatomical variants (such as trabeculae or LV false tendons).5,6 Cardiac myxomas are often found in the left atrium and are unlikely to be found in the LV. Cardiac tumors are often found in myocardium or endocardium. Vegetations are often found on valves. LV trabeculae are often found on the cardiac wall and can also mimic a left ventricular mass, but they typically have numerous partitions. LV false tendons are often thin, rectangular like-structures and are not spherical.
Despite having a presentation consistent with low-risk chest pain, in the setting of this patient’s extensive cardiac history, a bedside echocardiogram was completed in the ED to complete his chest pain workup identifying a left ventricular mass concerning for a thrombus. Had this thrombus not been found on bedside echocardiogram, it may have embolized, leading to morbidities such as a stroke or other end organ ischemia. This further highlights the importance of adding bedside ultrasound to work up those with chest pain in the ED.
References
- Nayak D, Aronow WS, Sukhija R, McClung JA, Monsen CE, Belkin RN. Comparison of frequency of left ventricular thrombi in patients with anterior wall versus non-anterior wall acute myocardial infarction treated with antithrombotic and antiplatelet therapy with or without coronary revascularization. Am J Cardiol. 2004;93(12):1529-1530. doi:10.1016/j.amjcard.2004.02.066
- Asinger RW, Mikell FL, Elsperger J, Hodges M. Incidence of Left-Ventricular Thrombosis after Acute Transmural Myocardial Infarction. N Engl J Med. 1981;305(6):297-302. doi:10.1056/NEJM198108063050601
- Turhan S, Ozcan OU, Erol C. Imaging of intracardiac thrombus. Cor Vasa. 2013;55(2):e176-e183. doi:https://doi.org/10.1016/j.crvasa.2013.02.005
- Saric M, Armour AC, Arnaout MS, et al. Guidelines for the Use of Echocardiography in the Evaluation of a Cardiac Source of Embolism. J Am Soc Echocardiogr. 2016;29(1):1-42. doi:10.1016/j.echo.2015.09.011
- Dinesh Kumar US, Shetty SP, Sujay KR, Wali M. Left ventricular mass: A tumor or a thrombus diagnostic dilemma. Ann Card Anaesth. 2016;19(4):728-732. doi:10.4103/0971-9784.191551
- Misumi I, Sato K, Nagano M, et al. Left Ventricular Apical Thrombus Mimicking Hypertrabeculation. Intern Med. 2021;60(14):2245-2250. doi:10.2169/internalmedicine.6482-20
Fellows Section:
Performing ultrasound-guided intercostal nerve blocks in patients with acute rib fracture pain
Rebecca G. Theophanous, MD MHSc FAAEM
Case presentation
An 85-year-old-male arrives to the emergency department via ambulance with chest wall pain after a mechanical fall from standing. He has a large contusion on his right posterior chest wall and is taking shallow quick breaths from the pain. His oxygen saturation is 91% on room air, so the patient is placed on two liters of supplemental oxygen. Chest x-ray shows multiple right-sided lower thoracic rib fractures and chest computed tomography scans reveals a right-sided apical pneumothorax. How can you help treat the patient’s pain without contributing to delirium and to prevent worsening of his respiratory symptoms and/or complications such as pneumonia?
Ultrasound-guided nerve blocks are a useful bedside tool for achieving more sustained pain control in settings of acute pain or trauma. The Intercostal Nerve Block (ICNB) is a relatively safe and easy-to-perform block that can improve pain control, potentially reduce delirium from medication adverse effects such as opioids, and can lessen or prevent complications in patients with acute rib fractures, especially in the elderly population.
Indications
ICNB is an appropriate method of regional anesthesia in patients with acute rib fracture pain, post-surgical pain after chest wall or upper abdominal surgery, or other causes of severe thoracic musculoskeletal pain. It is best used at the T7-T11 level due to the posterior approach because the scapula and rhomboid muscles are obstructive at higher levels (Figure 1). Thus, paravertebral or thoracic epidural blocks are likely better options for upper levels. ICNB is ideal for one-sided rib pain (either right or left) to avoid the very minimal possibility of bilateral pneumothorax and to avoid local anesthetic systemic toxicity given the higher amounts of anesthetic required. ICNB cannot be used for visceral pain from intra-abdominal organs.
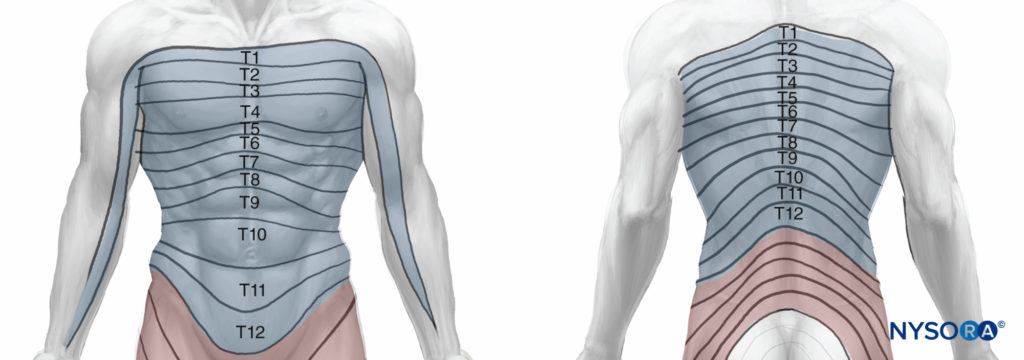
Figure 1: Anatomy. Source: NYSORA.COM
Contraindications
ICNB is contraindicated in patients on active anticoagulation, with severe bleeding risk, or with local infection overlying the potential area of needle insertion. Furthermore, it should only be performed after proper training and expertise, and with the appropriate equipment and cardiopulmonary monitoring in place.
Thoracic Anatomy
The neurovascular bundle is located inferior to each rib at the subcostal groove. The intercostal nerve lies caudal or inferior to the intercostal artery then vein (Figure 2). ICNB blocks the ipsilateral sensory and motor fibers of the ICNs. The ICN can be blocked anywhere proximal to the midaxillary line, where the lateral cutaneous branch takes off. The nerves typically can have additional innervation to the level above and below the respective rib space, and some may also enter the paravertebral space.
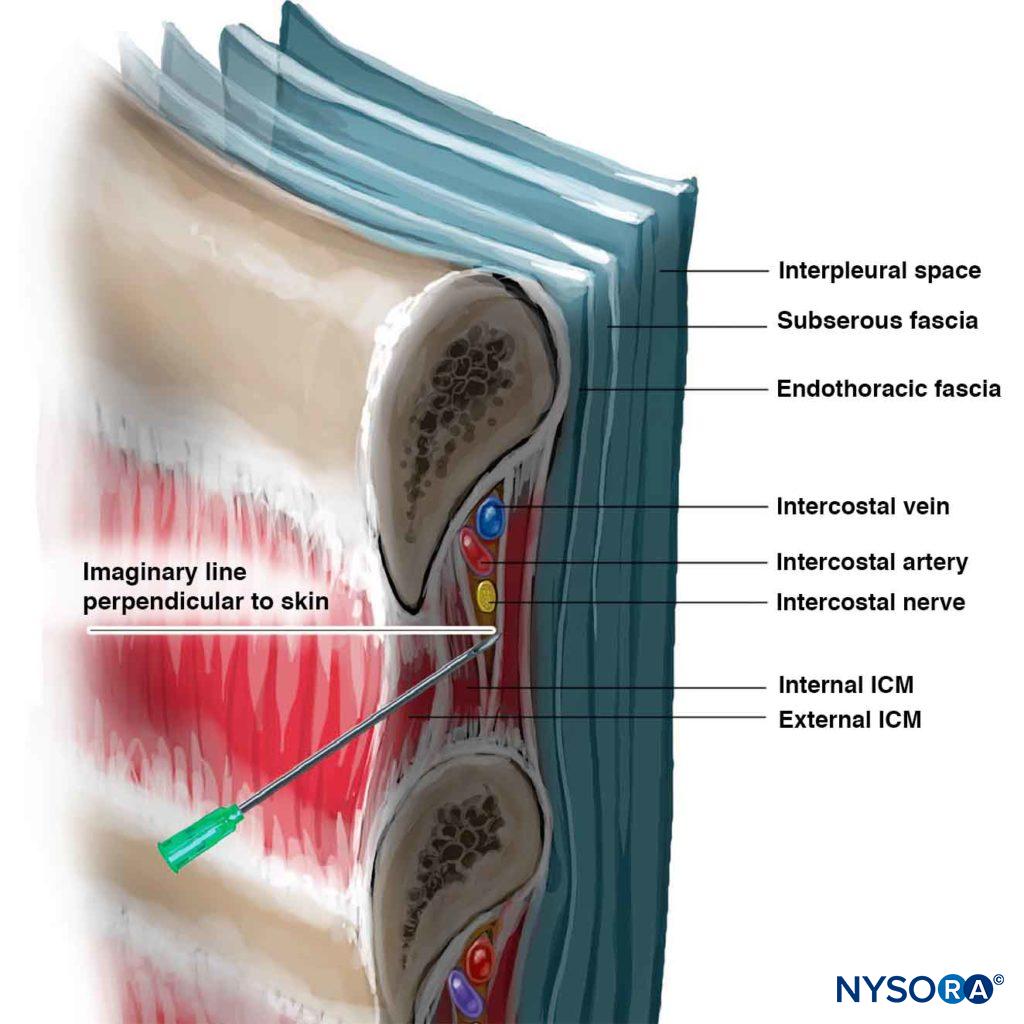
Figure 2: Nerve Bundle Anatomy. Source: NYSORA.COM
Suggested Equipment
- Ultrasound machine with high-frequency linear transducer (8-13 MHz)
- Antimicrobial skin cleanser
- Sterile and Personal Protective Equipment including gloves, gown, drapes, probe cover, sterile gel, etc.
- Marking pen
- 20G or 22G needle with 1.5inch length (4-5cm)
- Local anesthetic (e.g. lidocaine, bupivacaine, ropivacaine)
- Syringes (e.g. 3ml, 10ml, 20ml)
- Optional extension tubing between the needle and syringe if performing with an assistant
- 2×2 gauze and band-aids
- Cardiopulmonary monitors and resuscitative equipment (available in case of complication)
- Lipid emulsion 20% (available at bedside but should not need to be used)
Step-by-step approach and Technique
- Optimize patient positioning (Figure 3): the patient should be sitting upright with their arms hugging a pillow across a table and leaning slightly forward to retract the scapula. The patient should be attached to cardiopulmonary monitoring throughout the procedure with supplemental oxygen and intravenous lipid emulsion therapy available at the bedside. The skin should be cleaned with antiseptic solution and proper sterile technique used throughout the procedure.
- Mark landmarks (Figure 3): The inferior aspect of the pertinent 7th-11th ribs should be marked approximately 7cm away from the midline on the patient’s right or left back. The level of the pain or fracture should be marked, as well as the level above and below.

Figure 3: Landmarks. Source: NYSORA.COM
- Ultrasound probe position (Figure 4): To mark the ribs, the high-frequency linear transducer (8-13 Hz) should be oriented in a sagittal position to identify the external, internal, and innermost intercostal muscle layers between the two ribs, with the pleural space deep to these structures. Doppler or B mode should be used to visualize the blood vessel vascular flow to avoid these structures.
- Needle insertion (Figure 4): The needle should be inserted with the bevel pointing up and directed cephalad at a 20-degree angle in a similar plane with the ribs. The needle should be advanced slowly in-plane under ultrasound-guidance 1mm at a time at the inferior edge of the rib under the costal groove until the needle touches the bony periosteum.
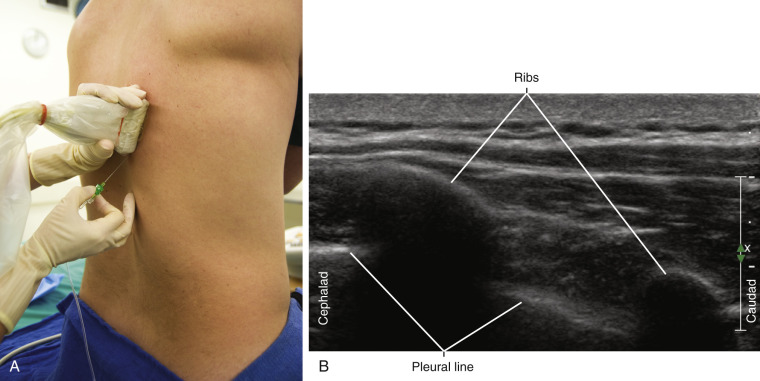
Figure 4: Needle positioning. Source: NYSORA.COM
- Local anesthetic injection (Figure 5): The assistant (or sole provider) should aspirate to ensure no blood return then inject a small amount of anesthetic at the periosteum. Then they should retract the needle and reapproach another 2-3mm inferior to the rib until a “pop” is felt when penetrating the fascia near the internal intercostal muscle. The patient may or may not feel paresthesia. Aspirate then inject 3-5mL anesthetic between the innermost intercostal muscle and the internal intercostal muscle layers, then retract the needle.
- Repeat the process at the rib level above and again at the level below, injecting 3-5mL at each level to maximize anesthetic effect.
Helpful Tip: A two-person technique can be used so that one person is introducing the needle under ultrasound-guidance while the other person is aspirating and injecting the anesthetic (Figure 6).
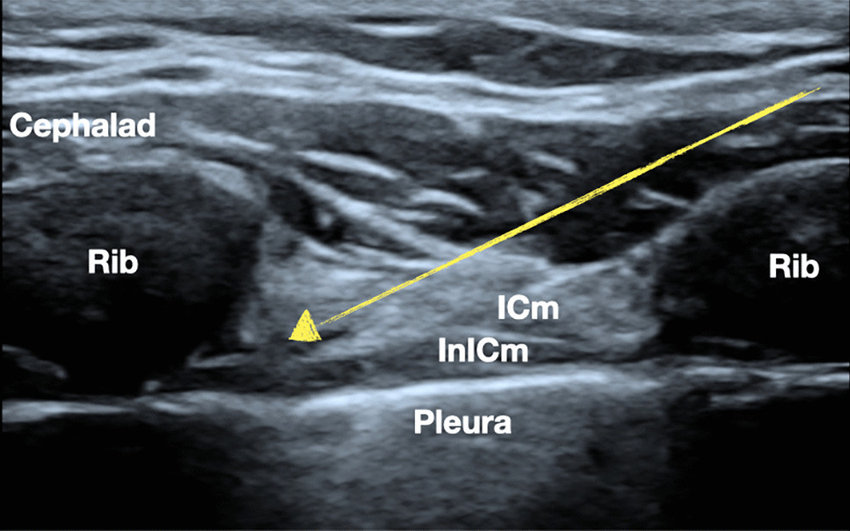
Figure 5L ICNB US image. Source: NYSORA.COM

Figure 6: Two person technique. Source: NYSORA.COM
Anesthetic medication properties
Local anesthetic medication options, dosing, and duration of action are listed in the following table. Typically, 3-5mL should be injected at the level above, at, and below the pain, with a dose of about 0.1 to 0.15 ml/kg per intercostal space. The addition of Epinephrine to Bupivacaine or Ropivacaine can increase the maximum injected dose by about 30% due to slower systemic absorption. Typical duration of action is 12 ± 6 hours.
| Anesthetic Medication Name | Concentration | Maximum Dosing | Duration of action |
| Lidocaine | 1% | 5 mg/kg/injection | 1-2 hours |
| Lidocaine w/ Epinephrine | 1-2% | 7 mg/kg/injection | 2-6 hours |
| Bupivacaine | 0.25-0.5% | 2-3 mg/kg/injection | 2-4 hours |
| Ropivacaine | 0.5% | 4 mg/kg/injection | 2-4 hours |
Potential complications
Arterial puncture, bleeding, infection, hemo/pneumothorax, and muscle laceration or injury are possible although rare if the procedure is performed under ultrasound-guidance with appropriate sterile technique, gradual needle advancement while in-plane, and aspiration for no blood return prior to anesthetic injection.
Local anesthetic systemic toxicity (LAST) is a possible complication that can be avoided with appropriate dosing and should be recognized early. Symptoms can include dizziness or light-headedness, tongue paresthesia, circumoral numbness, palpitations or tachycardia, agitation, nervousness, confusion, tinnitus, muscle twitches, seizures, and cardiac/neurological toxicity.
To summarize key points
- ICNB is best performed from the posterior approach, at levels T7-T11 due to the scapula and rhomboid muscles. Higher thoracic levels or bilateral rib fractures can be blocked using alternative techniques such as thoracic paravertebral or epidural nerve blocks.
- The patient should be appropriately positioned with the inferior aspect of each rib marked and ultrasound-guidance used throughout to minimize risk of complications.
- The ideal entry angle is 20 degrees cephalad with needle insertion inferior to the rib at the subcostal groove, approximately 7cm lateral to the midline.
- Aspiration prior to anesthetic injection is critical, with slow advancement in-plane and deposition of 3-5ml of anesthetic at the appropriate rib level, plus the level above and level below for best analgesia effects due to collateral innervation.
- The total amount of anesthetic to be injected should be calculated prior to the procedure start to prevent anesthetic toxicity. The patient should be attached to cardiopulmonary monitoring devices at all times, and intravenous lipid emulsion 20% therapy should be available at the bedside.
Patient case resolution: The patient and his family consented to a regional nerve block for improved pain management from his acute rib fractures. After stabilization with supplemental oxygen, ultrasound-guidance was used to perform an intercostal nerve block, and the patient was admitted to the intensive care unit for further treatment of his traumatic injuries.
References
- Ho AM, Buck R, Latmore M, et al. Intercostal Nerve Block – Landmarks and Nerve Stimulator Technique. Nysora 2023. https://www.nysora.com/topics/regional-anesthesia-for-specific-surgical-procedures/thorax/intercostal-nerve-block/
- Lopez-Rincon RM, Kumar V. Ultrasound-Guided Intercostal Nerve Block. [Updated 2022 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555900/
- Gray AT. Chapter 54 – Intercostal Nerve Block. Atlas of Ultrasound-Guided Regional Anesthesia (Third Edition). Elsevier. 2019: 233-238. ISBN 9780323509510. https://doi.org/10.1016/B978-0-323-50951-0.00054-2. https://www.sciencedirect.com/science/article/pii/B9780323509510000542#f0010.
- El-Boghdadly, K. and Wiles, M.D. (2019), Regional anaesthesia for rib fractures: too many choices, too little evidence. Anaesthesia, 74: 564-568. https://doi.org/10.1111/anae.14634. https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/anae.14634
- Collins JB, Song J, Mahabir RC. Onset and duration of intradermal mixtures of bupivacaine and lidocaine with epinephrine. Can J Plast Surg. 2013 Spring;21(1):51-3. doi: 10.1177/229255031302100112. PMID: 24431939; PMCID: PMC3891109. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3891109/#:~:text=Lidocaine%20is%20known%20to%20have,epinephrine%20(6%2C7).
- Lagan G, McLure HA: Review of local anaesthetic agents. Curr Anaesth Crit Care 2004;15:247–254.
Procedures Section:
Transgluteal Sciatic Nerve Block for Acute Sciatica Pain Control in the Emergency Department
Aakash Shah MD, Evan Yates MD
Introduction
Lower back pain (LBP) constitutes one of the most common emergency departments and a significant cause of disability worldwide. In the United States, LBP accounts for over 2 million ED visits which is over 3% of all chief complaints [1]. Of patient’s presenting to the ER for LBP, about 1/3 of them are related to sciatica [2]. Current management of these patients includes non-steroidal anti-inflammatories (NSAIDS), acetaminophen, lidocaine patches, steroids, opiates, benzodiazepines, and muscle relaxants. These interventions have variable efficacy and frequently are ineffective in controlling patient symptoms. The transgluteal sciatic nerve block (TGSNB) provides an alternative treatment modality for emergency medicine providers.
TGSNB has been used by regional anesthesiologist for both acute and chronic pain but has only recently been described and utilized in emergency medicine. Its safety and efficacy have only started to be described in emergency medicine literature for the treatment of refractory back pain [3].
Methods and Materials
As this case report is devoid of identifiable information, it is exempt from IRB review requirements as per New York City Health + Hospitals. The patient consented to the TGSNB.
Patient was placed in the lateral recumbent position with the unaffected side on the bed and his hip and knee slightly flexed (Figure 1). The patient was prepped in sterile fashion. The greater trochanter and ischial tuberosity were palpated. The curvilinear probe was placed between the anatomic landmarks to identify the hyperechoic sciatic nerve, deep to the gluteus maximus muscle (Figure 2). Attach 20-gauge spinal needle to 20cc syringe filled with 15cc of 0.5% bupivacaine. With a spinal needle, approach the sciatic nerve using the in-plane technique. The needle tip is placed along the longitudinal axis of the transducer. The needle tip is visualized during its trajectory to the sciatic nerve. Once the needle tip is adjacent to the sciatic nerve, aspirate to ensure there is no blood return. At this point with proper positioning, inject 7.5cc of bupivacaine to bathe the sciatic nerve and redirect needle tip to the other side of the sciatic nerve, aspirate, then inject the remaining 7.5cc of bupivacaine.
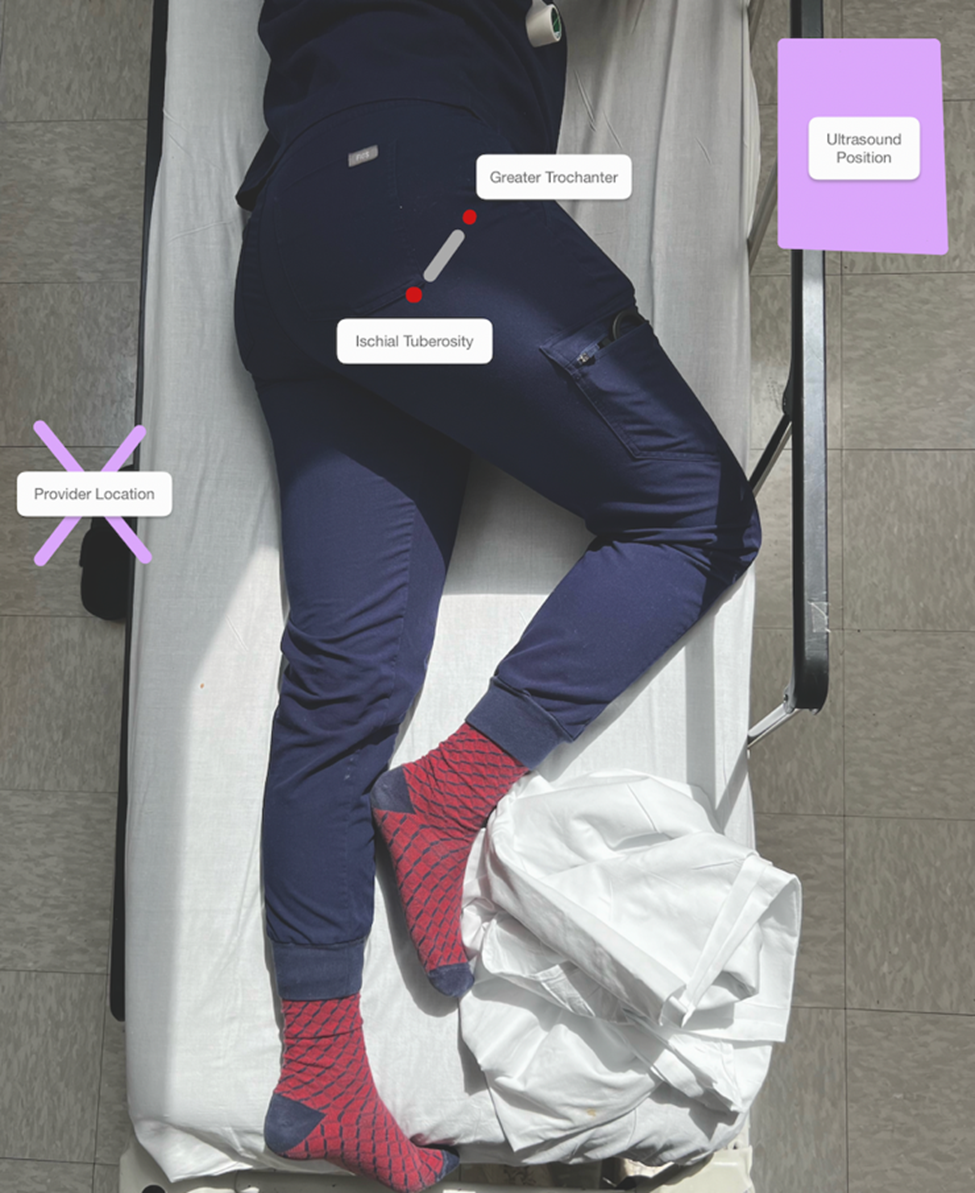
Figure 1: Positioning for TGSNB. Lateral Recumbent position with slight flexion at hip and knee.
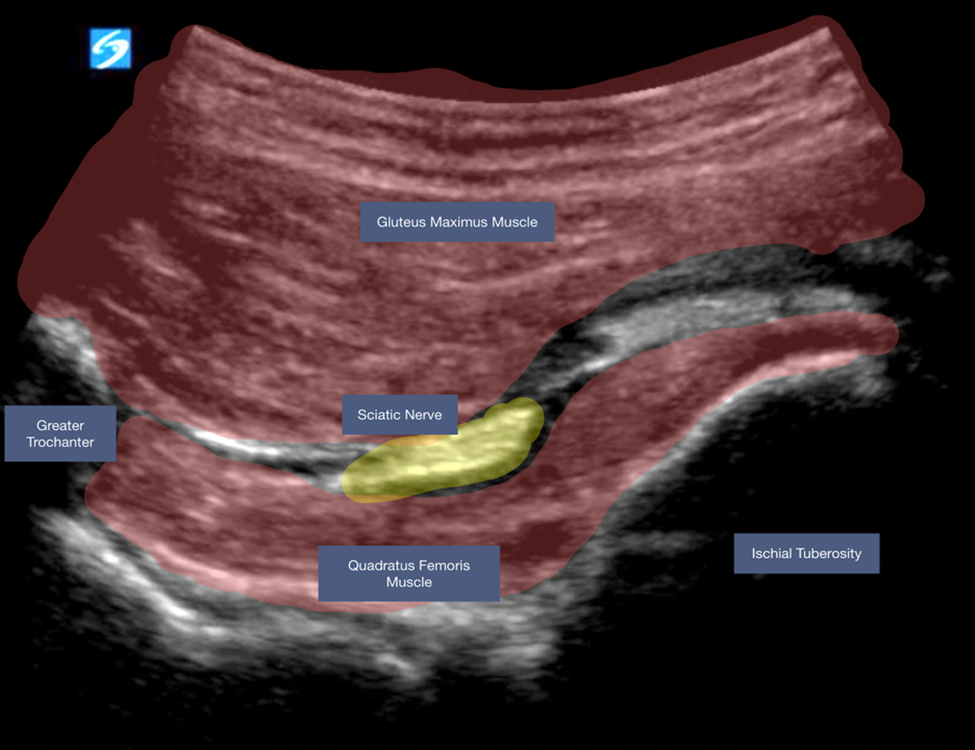
Figure 2: Ultrasound view with the sciatic nerve lying between Ischial Tuberosity and Greater Trochanter.
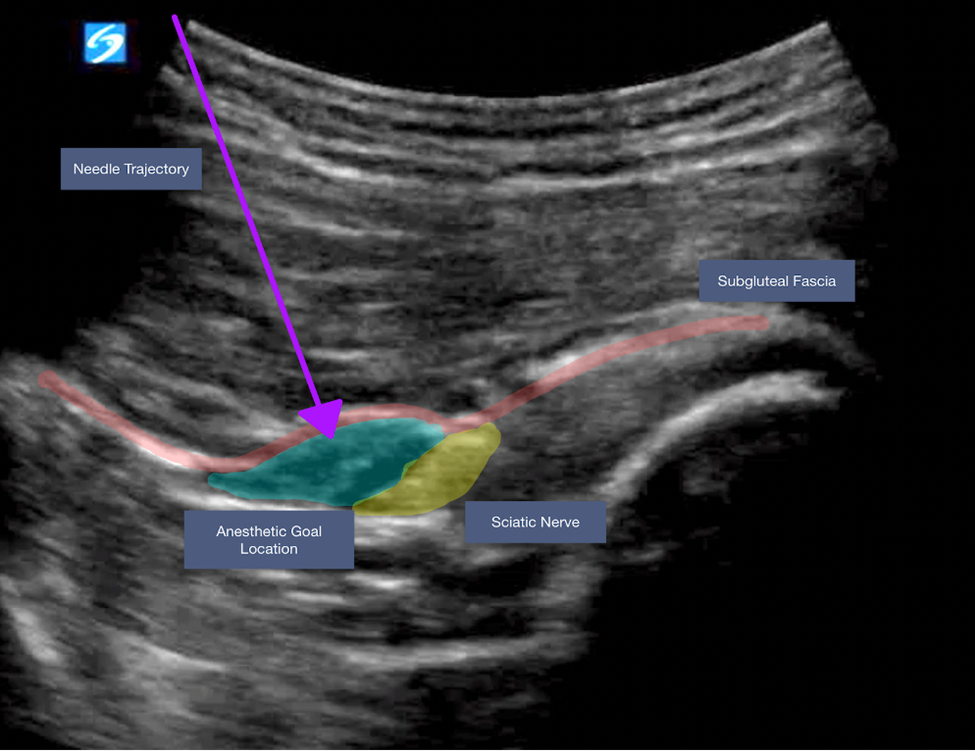
Figure 3: Annotated ultrasound image with arrow overlying needle trajectory.

Figure 4: Ultrasound view after anesthetic injection
Case Report
A 29-year-old man presented to the ED with acute on chronic lower back pain with radiation down his right posterior leg. He was previously a collegiate basketball player and reported known lumbar disc herniations. He was scheduled for outpatient neurosurgery clinic evaluation in the coming weeks. He had spent the previous day on a bus and since then had been having worsening lumbar pain, exacerbated with any movement. At baseline reported 8/10 pain that became 10/10 with attempted movement. Upon initial assessment he was able to ambulate no more than 6 steps without stopping in pain. He had a positive straight leg raise test on the right. He showed no neurologic deficits on the physical exam.
He was given NSAIDs, muscle relaxants, and a lidocaine patch which failed to improve his symptoms. Over the course of 2 hours, he also received acetaminophen, diazepam, and morphine without improvement in pain both subjectively and objectively with ambulation. He was then offered and consented for a TGSNB. Fifteen minutes after the TGSNB was performed, he reported 0/10 pain and was ambulating without discomfort around the emergency department. He was discharged shortly thereafter with follow up appointments to neurosurgery and chronic pain management. The patient was followed up at the 12, 24, and 36 hours mark to reassess patient pain level and functional status. At each time interval, the patient endorsed 0/10 pain, ability to conduct daily activities, and adverse effects were absent.
Discussion
The TGSNB provides a powerful and appropriate treatment modality for sciatica, especially in the emergency department setting, where there is no definitive intervention. In select patients, with known sciatica, it is an option that should be utilized by emergency providers. Overall, this nerve block is relatively safe and patients can have significant and/or complete resolution of symptoms. In this case, the multiple therapies were tried over hours, however, the patient had significant improvement shortly after the TGSNB.
In the limited studies published regarding TGSNB performed in the emergency room, all have been published by ultrasound trained faculty. However, technically, the block is easier to perform then many common blocks. The sciatic nerve is quite large and more easily visualized then other peripheral nerves. Secondly, there are no vascular structures that need to be avoided compared to many upper extremity nerve blocks. After developing proficiency, the TGSNB provides an efficient and safe modality of providing significant pain relief to patients with chronic lower back pain. While in this case, bupivacaine was the anesthetic chosen and administered alone, there are numerous alternatives described in the literature. Providers have described mixing normal saline, steroids, and/or utilizing alternative anesthetics. The selection is up to the provider.
Regarding the TGSNB, further studies could be performed to assess the efficacy of this intervention. Specifically, length of stay in the emergency department, bounce-back rates, follow-up to assess duration of pain relief. Theoretical adverse events include foot drop and anesthetic toxicity. However, from the case series describing TGSNB in the emergency department, there have not been any described adverse events. The limited studies have been performed by ultrasound trained emergency medicine physicians. The TGSNB shows promise in management of the acute pain exacerbations of patients with sciatica in the emergency department.
References
- Waterman B, Belmont P, Schonfeld A. Low back pain in the United States: incidence and risk factors for presentation in the emergency setting. Spine Journal. 2012 Jan;12(1):63-70.
- Nunn ML, Hayden JA, Magee K. Current management practices for patients presenting with low back pain to a large emergency department in Canada. BMC Musculoskelet Disord. 2017 Feb 23;18(1):92.
- Goldsmith AJ, Liteplo A, Hayes BD, Duggan N, Huang C, Shokoohi H. Ultrasound-guided transgluteal sciatic nerve analgesia for refractory back pain in the ED. Am J Emerg Med. 2020 Sep;38(9):1792-1795.