25TH ANNUAL SCIENTIFIC ASSEMBLY
MARCH 9-13, 2019 • CAESARS PALACE • LAS VEGAS, NV
MARCH 9-13, 2019 • CAESARS PALACE • LAS VEGAS, NV

Photographs of patients, pathology specimens, Gram stains, EKGs, and radiographic studies or other visual data may be submitted. Your submission should depict clear examples of findings that are relevant to the practice of emergency medicine or findings of unusual interest that have educational value. If your submission is accepted, you must mount it for viewing.
No more than three different photos may be submitted for any one case.
Eye Abnormality
Timmy Cheung, DO and Matthew J. Warner, MD FAAEM
Vineland, NJ
Photo submissions must include the following:
Please submit only blind copies, omitting your name, institution, city, state, or any other identifier.
Any photo that has been previously published or used in a national conference competition should not be submitted. Photos that have been presented at international meetings (MEMC) and have not been published, can be submitted for consideration.
If accepted for display, AAEM reserves the right to edit the submitted case history. Submissions are selected based on educational merit, relevance to emergency medicine, quality of the photograph, the case history, and appropriateness for public display. If your photograph is accepted, you will be notified and informed of set-up and dismantle times. Patients and patient identifiers must be appropriately masked. Additionally, you must attest that written consent and release of responsibility have been obtained for all photos EXCEPT for isolated diagnostic studies such as EKGs, radiographs, Gram stains, etc.
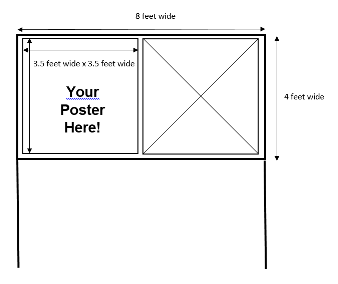
Responsibility for bringing photo and case submission(s) to the Scientific Assembly rests with the submitter. A 3.5´ x 3.5´ square area will be available for each submission. Photo competition participants who submit by 11:59pm CST on November 1, 2018, will receive notification of acceptance or rejection early January 2019.
|
|
 |
Christopher Scavelli, MD

Chief Complaint:
Rectal foreign body
History of Present Illness:
73 year old male with past medical history of hypertension, diabetes, hyperlipidemia, heart failure with reduced EF presented to ED with complaint of rectal foreign body. Patient states his wife inserted a light bulb into his rectum during sexual intercourse approximately 1 hour prior to arrival and was unable to remove it, despite use of pliers. Patient states he has had a similar episode in the past requiring administration of paralytics in OR for removal. Patient reports mild rectal pain at this time, denies other complaint.
Physical Exam:
VITALS: T-98.1, HR-79, BP-121/58, RR-20, SpO2-96%
GEN: alert and oriented, well-appearing, no apparent distress
CV: normal S1S2 without murmur, rub, or gallop
RESP: lungs clear to auscultation bilaterally without wheezes, rales, or rhonchi
GI: abdomen soft, non-tender, non-distended, normoactive bowel sounds, +cylindrical metal object approximately 4x3cm protruding from anus, no visible anal lacerations or abrasions, normal rectal tone
SKIN: warm and dry without rash
Questions:
Answers:

Case Discussion:
The patient was placed in an available resuscitation bay and only necessary providers (ED attending, two ED residents, ED nurse) were present to maximize the patient’s privacy. Particular attention was paid to addressing the patient’s embarrassment, as he was medically stable and his physical pain was minimal. A pelvic x-ray was obtained to further illustrate the nature of the object and help assess whether it remained intact. Imaging demonstrated what appeared to be a large incandescent light bulb, with the globe oriented cephalad and the base oriented caudad.
Consent was obtained from the patient to attempt foreign body removal. He was connected to a cardiac monitor, given Midazolam 2mg IV, and placed in the lithotomy position. Lubricant was applied to the patient’s anus and metal base of the light bulb. Constant firm manual traction was applied with some slight removal of base. The patient required two additional doses of Midazolam 2mg IV, though further attempts at manual removal were unsuccessful.
There was concern for accidental shattering of the glass bulb or removal of the globe from light bulb base, which limited the amount of manual traction applied. Attempts at introducing a flexible catheter rectally to traverse beyond the obstruction were considered to release presumed vacuum-effect, though the border between the rectal ampulla and the globe was impassable. There was also consideration of obtaining a light socket to obtain better external purchase of the light bulb by screwing in the base, but the risks of causing further local trauma or destruction of the bulb (impairing further removal efforts) were deemed too great.
General Surgery was consulted for examination under anesthesia, in the hopes that administration of paralytics may resolve the obstruction. The patient was brought to the OR and examination under general anesthesia was performed. Intra-operative efforts at manual removal also failed, despite use of paralytics. A loop descending colostomy was performed, which reportedly caused a release of pressure. Examination under anesthesia was repeated with successful removal of an 18 x 7cm incandescent light bulb.
Pearls:
If you have questions regarding the abstract submissions for the 25th Annual Scientific Assembly, please call Rebecca Sommer at (800) 884-2236 or email rsommer@aaem.org.